Hypertension artérielle
De médecine.top
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
Hypertension artérielle sévère
Urgence hypertensive hypertensive emergency
Pression artérielle élevée et dommage d'organe/dysfonction associée
Recommandations
- For adults with a hypertensive emergency and a compelling condition (such as aortic dissection, severe preeclampsia or eclampsia, or pheochromocytoma crisis), systolic blood pressure should be reduced to less than 140 mm Hg during the first hour and to less than 120 mm Hg in aortic dissection.
- For adults with a hypertensive emergency but without a compelling condition, systolic blood pressure should be reduced by no more than 25% within the first hour; then, if stable, to 160/100 mm Hg within the next 2 to 6 hours; and then cautiously to normal during the following 24 to 48 hours.[1]
Crise hypertensive hypertensive urgency
texte
Hypertension artérielle primaire (essentielle)
Diagnostic
- Au cabinet: première visite → position assise, manchette adaptée, TA aux 2 bras (valeur la plus haute prise en compte), tranquillité 5 min, 3 mesures de la pression à 1-2 min intervalle, moyenne des 2 dernières mesures
- En ambulatoire: mesure ambulatoire de la pression artérielle (MAPA), Remler)
Classification ESC 2018

Bilan
- Recherche d'atteinte d'organe cible:
| Paramètre | Remarque |
|---|---|
| Créatininémie | |
| Créatininurie et albuminurie | Rapport albuminurie/créatininurie ACR [mg/g] |
| ECG | Signes d'hypertrophie ventriculaire gauche |
| Echocardiographie | |
| US doppler des artères rénales | Exclusion d'une sténose, bilan aorte, mesure index résistances rénales |
| (Bilan lipidique: LDL-cholestérol, HDL-cholestérol, triglycérides) | Calcul du risque cardiovasculaire |
- Calcul du score de risque cardiovasculaire:
- GSLA https://www.agla.ch/fr/calculateurs-outils/calculateur-de-risque-du-gsla
- SCORE https://www.heartscore.org → recommandations ESC 2018
Traitement
- Modifications non médicamenteuses: arrêt du tabac, perte de poids avec cible BMI <25, restriction sodée, diète DASH avec apports en potassium, augmentation des fruits et légumes
- Traitement médicamenteux:
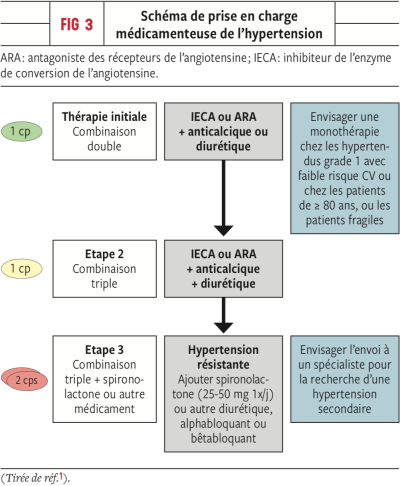 Source: Rev Med Suisse 2019 ; 15 : 57-61
Source: Rev Med Suisse 2019 ; 15 : 57-61- Indication:
- Patients de 18-79 ans: indication au traitement médicamenteux dès HTA de grade 1 (140/90 mmHg) quelles que soient les maladies associées (diabète, insuffisance rénale, maladie coronarienne, AVC)
- Patients ≥80 ans: dès 160/90 mmHg
- Patients à risque cardiovasculaire élevé
- diurétique thiazidique (hydrochlorothiazide), chlortalidone
- Alternative: Loop diuretics are preferred in patients with symptomatic heart failure or CKD with an estimated GFR <30 mL/min/1.73 m2. Potassium-sparing diuretics, such as aldosterone receptor antagonists (spironolactone or eplerenone) or epithelial sodium channel blockers (amiloride), are weaker diuretics. These are often used in liver cirrhosis, heart failure, or resistant hypertension.
- The 2017 ACC/AHA BP guideline recommends combination therapy with two first-line antihypertensive drugs of different classes for adults with stage 2 hypertension and an average BP of 20/10 mm Hg above their BP target (typically ≥150/90 mm Hg).
- Thérapies adjonctives:
- β-blockers for post–myocardial infarction or heart failure
- aldosterone receptor blockers for heart failure
- loop diuretics for advanced CKD
